

A more proactive approach to T2D treatment from the initial diagnosis can support early glycemic control1
Proactive treatment is an approach consistent with ADA/EASD recommendations to reassess patients who are not at glycemic goal every 3 months (or additionally as required for safety)1,15
Treat at the Point of Failure, or a stepwise approach where medication is changed only when symptoms become apparent rather than when glycemic targets fall outside of recommended guidelines, is often a barrier to sustained glycemic control.15
Schematic illustrations depicting hypothetical treatment scenarios1,15,16
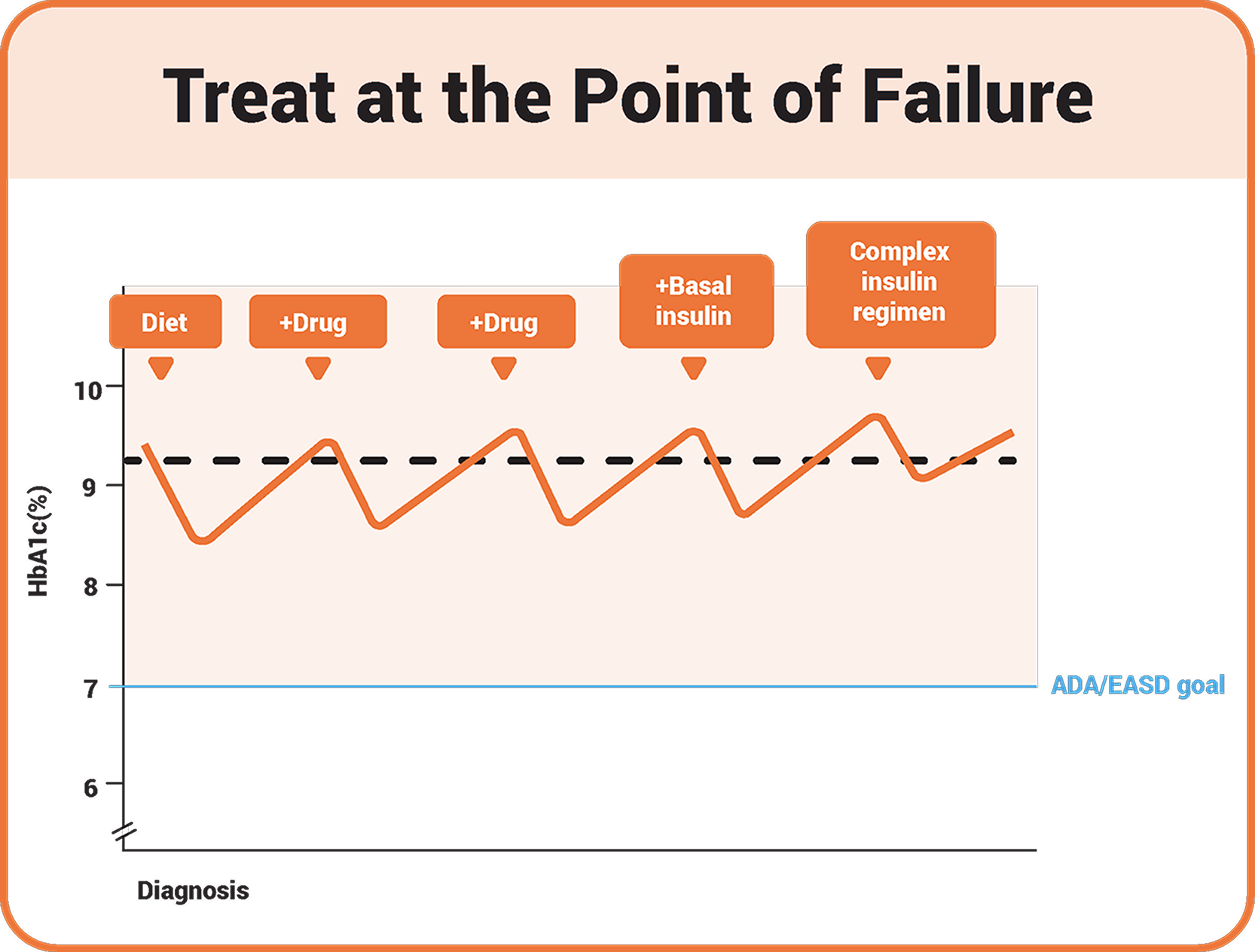
The line diagram shows treatment up to the point of treatment failure. The HbA1c value is briefly reduced by various interventions when symptoms occur, but then rises again. The target value of ADA/EASD is not achieved by the interventions.
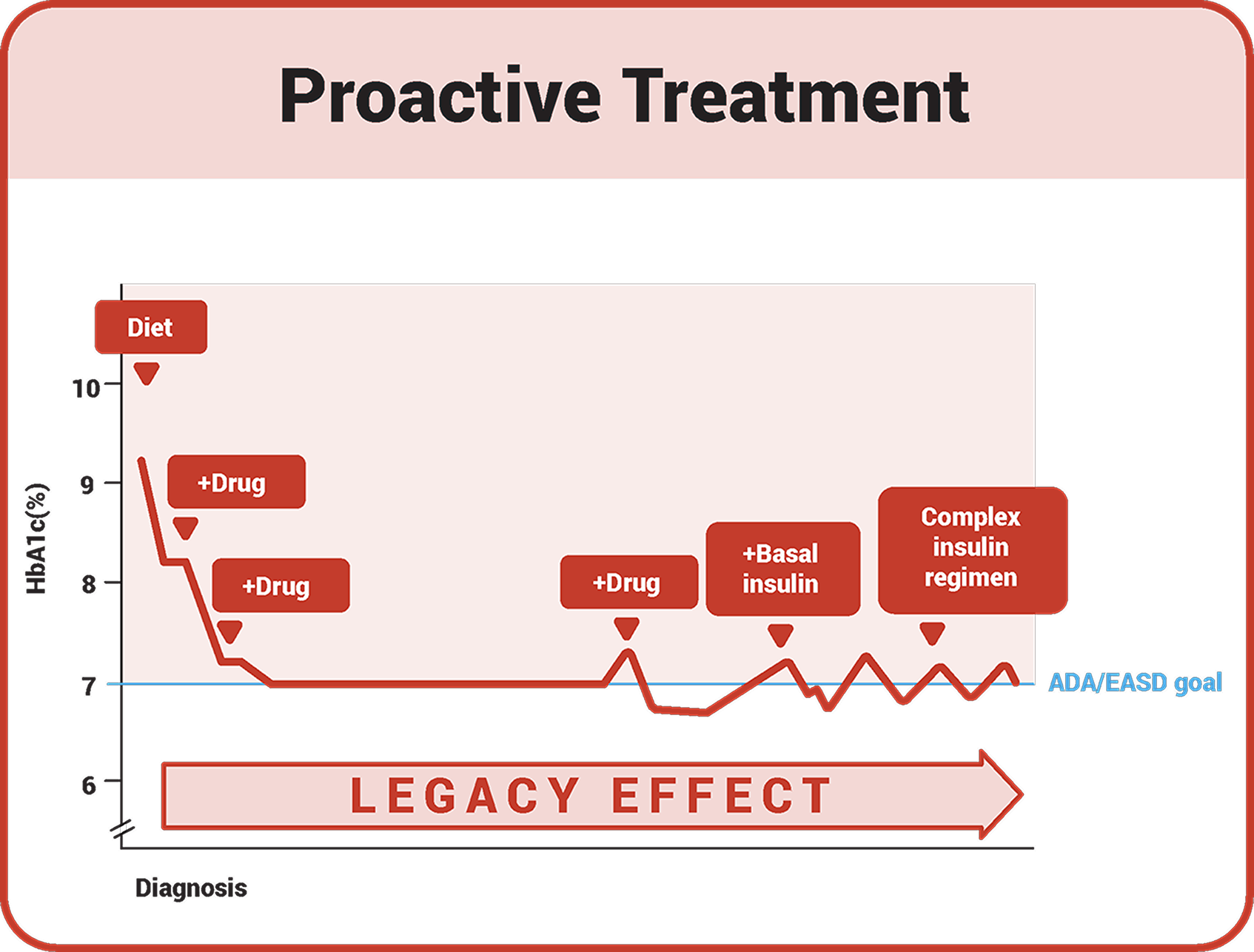
The line graph shows targeted treatment. Targeted treatment when the ADA/EASD target value is exceeded enables patients to achieve the target value again and again with the help of various interventions. Early therapy leads to the legacy effect.
The benefits of a more proactive approach to treatment have been described in clinical trials1,15-17
In the 5-year VERIFY clinical trial, early combination treatment targeting multiple defects reduces time to initial and secondary treatment failures compared with a conventional stepwise approach.17‡
With early combination therapy (vildagliptin/metformin), patients experienced17:
- 49% relative risk reduction in time to initial treatment failure vs metformin alone17
- 26% relative risk reduction in time to secondary treatment failure with initial combination therapy vs sequential addition of treatment17
- 5 years median time to escalate to insulin with initial combination therapy vs 3 years with a conventional stepwise approach17
‡VERIFY was a 5-year, randomized, 1:1, double-blind, parallel-group study (n≈2000) designed to compare early initiation of a vildagliptin-metformin combination with standard-of-care initiation of metformin monotherapy, followed by the stepwise addition of vildagliptin when glycemia deteriorated. Participants with further deterioration were treated with insulin. Treatment failure was defined as a loss of glycemic control (2 consecutive values of HbA1c ≥7%).17,18
Proactive treatment, which can include targeting multiple defects early and combination treatment, can result in superior glycemic control and has the potential to improve long-term T2D-related outcomes.1,15-17
A stepwise approach has previously been the standard for treating patients with T2D. In the 2022 ADA/EASD Consensus report, a proactive and individualized approach, including choosing high or very high efficacy treatment, should be used to support people with T2D in achieving their treatment goals.1,15

ADA Standard of Care19:
“Patients not at goal with treatment adjustments may require testing more frequently (every 3 months with interim assessments as needed for safety).”
The schematic is intended to provide an overview of T2D drugs and is not specific to only 1 product within each class listed. It is not limited to making any expressed or implied comparison among products. The classes shown are from the ADA Standards of Care and do not represent all T2D classes available to treat hyperglycemia.
Let's check in on Ahmed!
At his initial diagnosis, Ahmed was prescribed metformin and lifestyle modifications. Following the guidelines, Ahmed's treatment was intensified at his 3-month check-in because his HbA1c was still above target at 7.2%, and he continued to have excess weight. A treatment that is effective for both glycemic control and weight management was chosen, supporting his lifestyle changes.1

Proactive Treatment
After 1 year of follow-up appointments every 3 months to assess results or to make treatment adjustments as needed, Ahmed saw results that he could feel good about and is hopeful about his future with T2D.

Development of Ahmed's HbA1c value and weight. At initial diagnosis, the HbA1c value was 7.8% and the BMI was 29 kg/m2. After three months, the HbA1c value was 7.2% and the BMI was 29.5 kg/m2. Based on these values, the therapy was intensified. After 6 months, the HbA1c value was 6.5% and the BMI was 28 kg/m2. After 9 months, the HbA1c value was 6.3% and the BMI was 26.5 kg/m2. After 12 months, the HbA1c value was 6.4% and the BMI was 26 kg/m2.
How might Ahmed’s results look without early treatment intensification?
In many cases, patients like Ahmed do not have their medication intensified at the first sign that greater glycemic control will be needed. Observational trials have shown that many patients like Ahmed remain on metformin alone for over a year. Ahmed’s treatment journey could have looked very different if his treatment had not been intensified in that first follow-up.15,17,20
Treat at the Point of Failure
In this scenario, Ahmed remained on metformin at his 3-month follow-up, and his dosage was increased at his 6-month follow-up as he remained slightly above target. At his 1-year follow-up, he had not yet achieved his glycemic goals.20

Course of Ahmed's HbA1c value and weight when treatment was continued until it failed. At initial diagnosis, the HbA1c value was 7.8% and the BMI was 29 kg/m2. After three months, the HbA1c value was 7.2% and the BMI was 29.5 kg/m2. After 6 months, the HbA1c value was 7.5% and the BMI was 29.7 kg/m2. Based on these values, the metformin dose was increased. After 9 months, no values were available. After 12 months, the HbA1c value was 8.1% and the BMI was 30.1 kg/m2

How do these 2 treatment approaches compare? What long-term outcomes should be considered when making early treatment decisions?
- Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes,2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753-2786.doi:10.2337/dci22-0034
- Kendall DM, Cuddihy RM, Bergenstal RM. Clinical application of incretin-based therapy:therapeutic potential, patient selection and clinical use. Am J Med. 2009;122(6 suppl):41S37-S50. doi:10.1016/j.amjmed.2009.03.015
- Schwartz SS, Epstein S, Corkey BE, et al. The time is right for a new classification system for diabetes: rationale and implications of the β-cell-centric classification schema. Diabetes Care. 2016;39(2):179-186. doi:10.2337/dc15-1585
- UK Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837-853. doi:10.1016/S0140-6736(98)07019-6
- DeFronzo RA. Banting Lecture. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes. 2009;58(4):773-795.doi:10.2337/db09-9028
- Chait A, den Hartigh LJ. Adipose tissue distribution, inflammation and its metabolic consequences, including diabetes and cardiovascular disease. Front Cardiovasc Med. 2020;7:22. doi:10.3389/fcvm.2020.00022
- de Luca C, Olefsky JM. Inflammation and insulin resistance. FEBS Lett. 2008;582(1):97-105. doi:10.1016/j.febslet.2007.11.057
- Xu H, Barnes GT, Yang Q, et al. Chronic inflammation in fat plays a crucial role in the development of obesity-related insulin resistance. J Clin Invest. 2003;112(12):1821-1830.doi:10.1172/JCI19451
- Trouwborst I, Bowser SM, Goossens GH, Blaak EE. Ectopic fat accumulation in distinct insulin resistant phenotypes; targets for personalized nutritional interventions. Front Nutr. 2018;5:77. doi:10.3389/fnut.2018.00077
- Raji A, Seely EW, Arky RA, Simonson DC. Body fat distribution and insulin resistance in healthy Asian Indians and Caucasians. J Clin Endocrinol Metab. 2001;86(11):5366-5371. doi:10.1210/jcem.86.11.7992
- Kozawa J, Shimomura I. Ectopic fat accumulation in pancreas and heart. J Clin Med. 2021;10(6):1326. doi:10.3390/jcm10061326
- Ye R, Onodera T, Scherer PE. Lipotoxicity and β cell maintenance in obesity and type 2 diabetes. J Endocr Soc. 2019;3(3):617-631. doi:10.1210/js.2018-00372
- Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015;38(1):140-149. doi:10.2337/dc14-2441
- Mounjaro (tirzepatide once weekly) [Summary of Product Characteristics]. Houten, The Netherlands: Eli Lilly and Company.
- Campbell IW. Need for intensive, early glycemic control in patients with type 2 diabetes. J Brit Cardiol. 2000;7:625-631.
- Holman RR, Paul SK, Bethel MA, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577-1589. doi:10.1056/NEJMoa0806470
- Matthews D, Del Prato S, Mohan V, et al. Insights from VERIFY: early combination therapy provides better glycaemic durability than a stepwise approach in newly diagnosed type 2 diabetes. Diabetes Ther. 2020;11(11):2465-2476.doi:10.1007/s13300-020-00926-742
- Del Prato S, Foley JE, Kothny W, et al. Study to determine the durability of glycaemic control with early treatment with a vildagliptin-metformin combination regimen vs. standard-of-care metformin monotherapy—the VERIFY trial: a randomized double-blind trial. Diabet Med. 2014;31(10):1178-1184. doi:10.1111/dme.12508
- American Diabetes Association Professional Practice Committee. 6. Glycemic targets: Standards of Medical Care in Diabetes—2022. Diabetes Care. 2022;45(suppl 1):S83-S96.
- Gomes MB, Rathmann W, Charbonnel B, et al. Treatment of type 2 diabetes mellitus worldwide: baseline patient characteristics in the global DISCOVER study. Diabetes Res Clin Pract. 2019;151:20-32. doi:10.1016/j.diabres.2019.03.024
- Lind M, Imberg H, Coleman RL, et al. Historical HbA1c values may explain the type 2 diabetes legacy effect: UKPDS 88. Diabetes Care. 2021;44(10):2231-2237.doi:10.2337/dc20-2439
- Laiteerapong N, Ham SA, Gao Y, et al. The legacy effect in type 2 diabetes: impact of early glycemic control on future complications (The Diabetes & Aging Study). Diabetes Care. 2019;42(3):416-426. doi:10.2337/dc17-1144