

Obesity and Its Complications
Obesity is a chronic disease characterized by increased adiposity (excess fat), which can lead to numerous health problems1
Adipocyte (fat cell) dysfunction is a main driver of many obesity-related metabolic complications2
Adipose tissue has long been misunderstood as just a storage organ for energy. However, with the rise of obesity, adipose tissue is now being recognized as an essential organ in regulating energy homeostasis.2
Adipocytes become dysfunctional in people with obesity. These adipocytes are not able to properly store excess energy, leading to fat deposition in ectopic and visceral locations in turn causing inflammation and metabolic abnormalities.2,3

The hypothalamus controls the homeostatic food intake and influences the feeling of satiety, appetite and energy metabolism. The mesolimbic system controls hedonic food intake and is responsible for preferences and desires. The prefrontal cortex has an executive function. It takes over self-regulation and inhibitory control. Satiety and hunger can be influenced by various hormones. Intestinal hormones (GLP-1, CCK, GIP), adipose tissue hormones (leptin) and pancreatic hormones (amylin and insulin) affect the feeling of satiety; a stomach hormone (ghrelin) affects the feeling of hunger.
IL-6=interleukin 6; MCP-1=monocyte chemoattractant protein-1; TNF-α=tumor necrosis factor alpha.
Obesity affects multiple organ systems and is responsible for more than 200 complications5,6
Complications occur through multiple effects of adiposity6,7
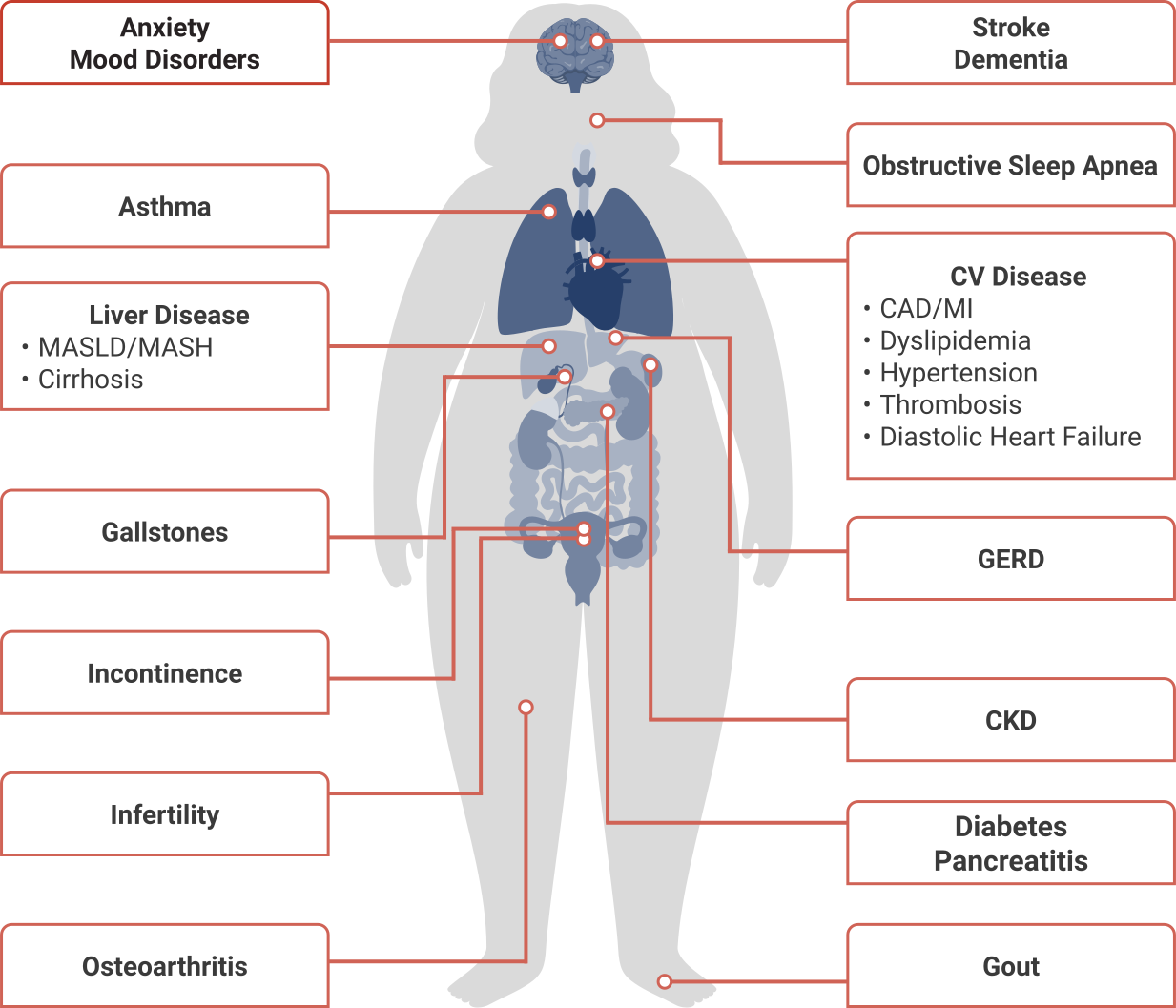
The graphic shows a human body and gives an overview of possible complications and secondary diseases of obesity. These include: anxiety, mood disorders, asthma, liver disease (MASLD/MASH), gallstones, incontinence, infertility, osteoarthritis, stroke, dementia, obstructive sleep apnea, cardiovascular diseases (coronary heart disease/myocardial infarction, dyslipidemia, hypertension, thrombosis, diastolic heart failure), gastroesophageal reflux, chronic kidney failure, diabetes, pancreatitis and gout.
Weight reduction in people with obesity can improve long-term health outcomes8
Treating obesity may prevent the onset or progression of associated complications8-10
Prioritizing the treatment of obesity can have a positive impact on patients’ overall health and well-being.1,5,7
CAD=coronary artery disease; CKD=chronic kidney disease; CV=cardiovascular; GERD=gastroesophageal reflux disease; MI=myocardial infarction; MASH=metabolic dysfunction-associated steatohepatitis; MASLD=metabolic dysfunction-associated steatotic liver disease.
Obesity is connected to many other serious diseases5,8-10
Obesity can affect almost all organ systems and is associated with over 200 complications, some of which can be improved with weight loss.5,6

Type 2 Diabetes (T2D)
- Inflammation and dysfunctional lipid handling can lead to lipid deposition in organs such as liver, skeletal muscle, and heart. This ultimately leads to systemic inflammation and insulin resistance2
- Weight loss of ≥5% can support prevention of T2D5,9
- Weight loss of ≥10% can support remission of T2D5,9

Cardiovascular Disease (CVD)
- Obesity and increased adipose tissue, particularly in ectopic locations, influence the pathogenesis of atherosclerosis7,11
- In clinical studies, weight loss of >10% has been associated with a reduced risk of cardiovascular disease12
Obstructive Sleep Apnea (OSA)
- >70% of people with obesity have OSA13,14
- Obesity may worsen OSA because of fat deposition at specific sites, including the upper airway and thorax13
- Weight loss of ≥10% is associated with significant improvement in OSA12,13

Metabolic Dysfunction-Associated Steatotic Liver Disease/Metabolic Dysfunction-Associated Steatohepatitis (MASLD/MASH)
- Obesity occurs in 51% of people with MASLD (formerly known as NAFLD)25
- MASH (formerly known as NASH) occurs in 15% to 20% of PwO14
- Weight loss of ≥10% has been associated with progressive improvement in MASH14
- Over 90% of patients with severe obesity undergoing bariatric surgery have MASLD25

Polycystic Ovary Syndrome (PCOS)
- Obesity occurs in 30% to 75% of women with PCOS14
- Central adiposity is an independent risk factor associated with PCOS, and women with PCOS are more likely to have metabolic syndrome14
- Weight loss of 5% to 10% has been shown to improve PCOS5
Consider treatment for obesity to reduce the risk of complications
How the body resists weight reduction
The brain plays a key role in regulating energy balance through its effects on caloric intake and energy expenditure15
Energy homeostasis is centrally regulated by the brain.1,16
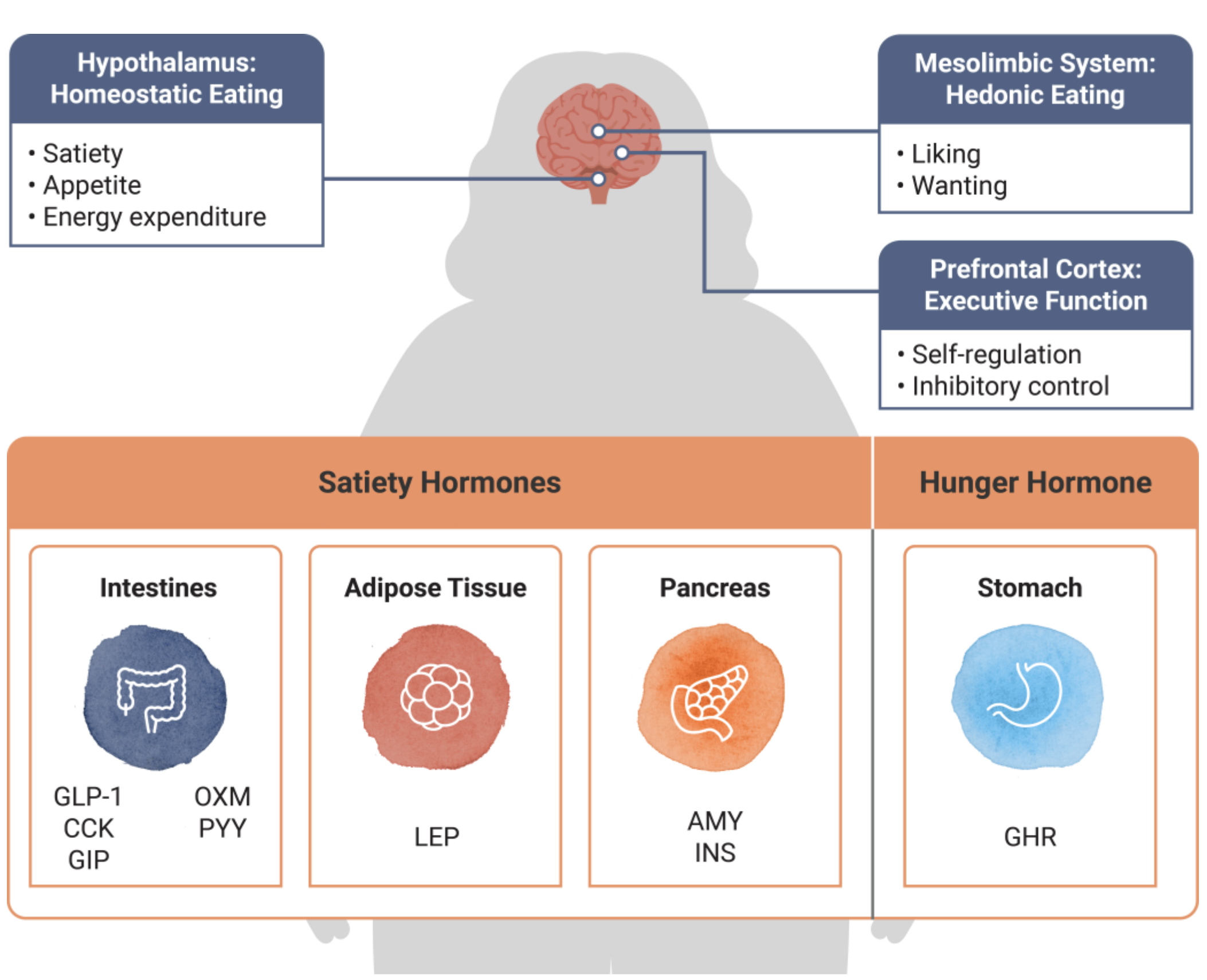
The hypothalamus controls the homeostatic food intake and influences the feeling of satiety, appetite and energy metabolism. The mesolimbic system controls hedonic food intake and is responsible for preferences and desires. The prefrontal cortex has an executive function. It takes over self-regulation and inhibitory control. Satiety and hunger can be influenced by various hormones. Intestinal hormones (GLP-1, CCK, GIP), adipose tissue hormones (leptin) and pancreatic hormones (amylin and insulin) affect the feeling of satiety; a stomach hormone (ghrelin) affects the feeling of hunger.
AMY=amylin; CCK=cholecystokinin; GHR=ghrelin; GIP=glucose-dependent insulinotropic polypeptide; GLP-1=glucagon-like peptide-1; INS=insulin; LEP=leptin; OXM=oxyntomodulin; PYY=peptide YY.
Weight loss can trigger adaptive changes in hunger and satiety hormones that favor weight regain and can persist for at least 1 year19
Biological Adaptations to Weight Loss18,20,21
- Increase in ghrelin (hunger hormone)
- Decrease in satiety hormones such as GLP-1
- Reduction in energy expenditure
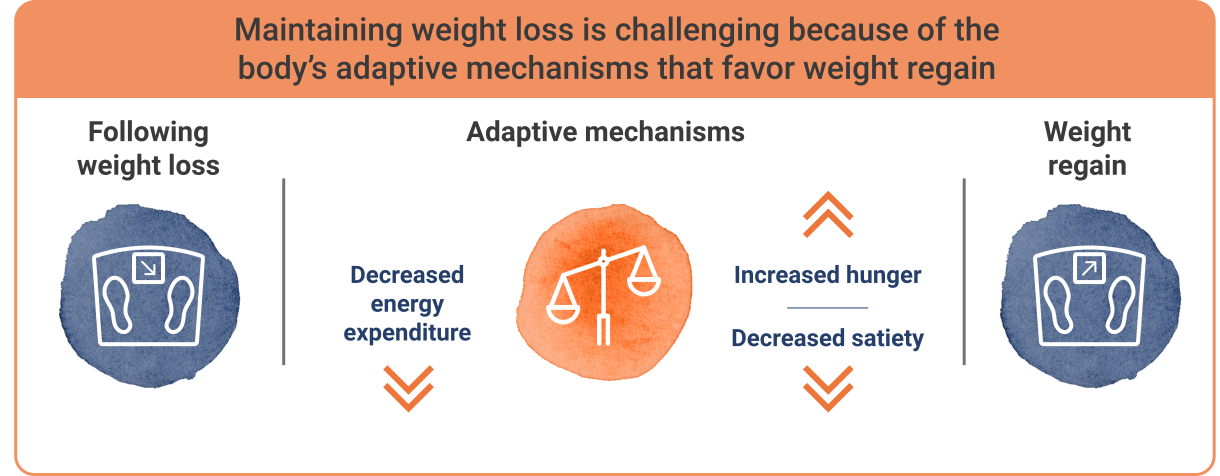
The graphic shows why it can be challenging to maintain weight after weight loss. After weight loss, the body's adaptive mechanisms can lead to reduced energy expenditure, increased hunger and reduced satiety. The result is renewed weight gain.
Ending the Stigma of Obesity
There is a widespread assumption that diet and exercise can entirely reverse obesity over long periods of time. This belief contradicts the indisputable scientific evidence demonstrating that voluntary efforts to reduce body weight activate biologic responses (eg, increased appetite and decreased metabolic rate) that typically promote long-term weight regain.22
Following weight loss, up to 79% is regained over time23,24
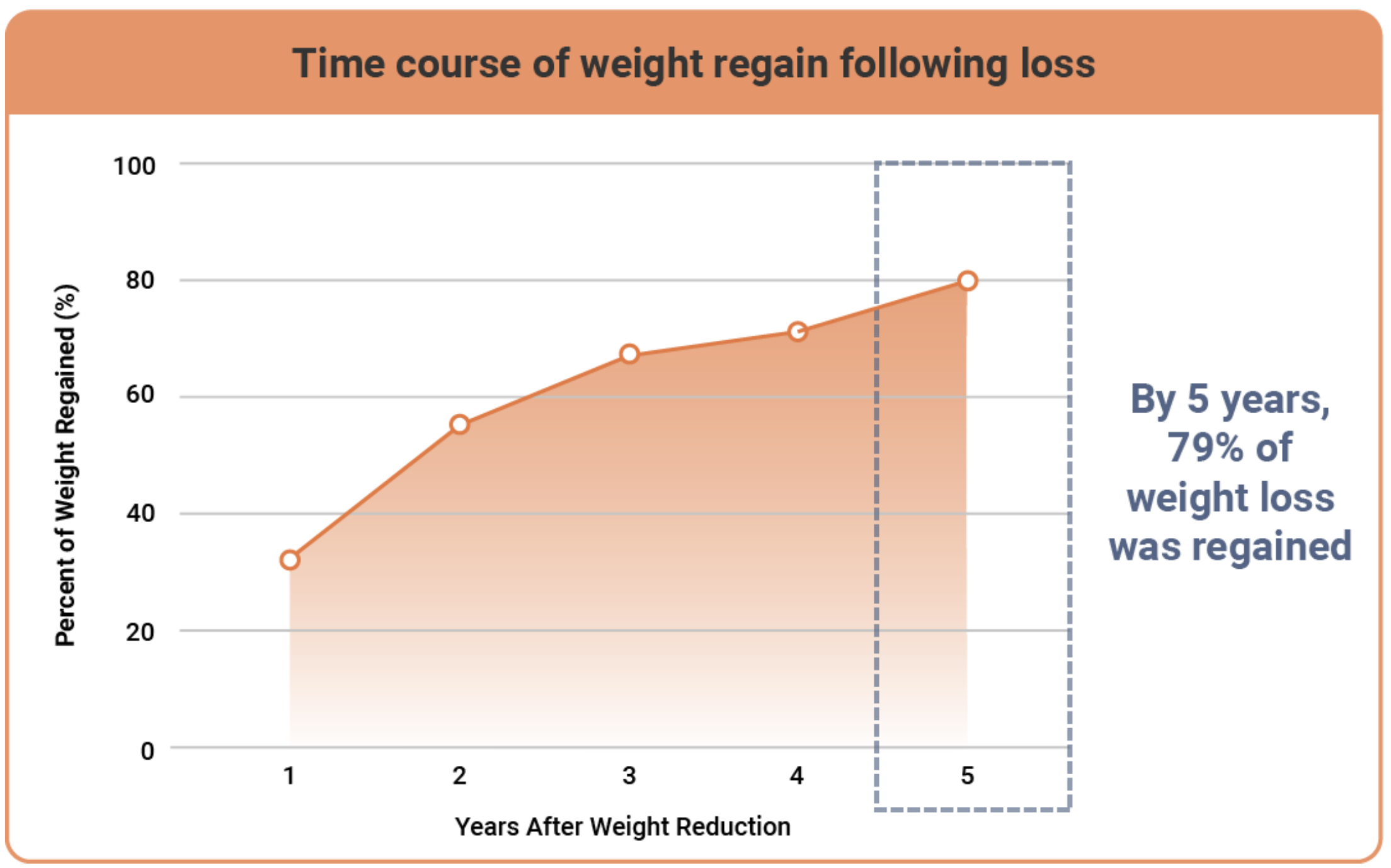
The line graph shows the course of weight gain after weight loss over a period of 5 years. Weight gain increases continuously after weight loss, so that after 5 years the participants had regained 79% of their lost weight.
A meta-analysis of 29 studies utilizing lifestyle modification as part of a structured weight-loss program indicated that by 4 or 5 years after initial weight reduction, the average individual regained 77% of weight lost, maintaining an average weight reduction of just 3% below initial weight.23
- Wharton S, Lau DCW, Vallis M, et al. Obesity in adults: a clinical practice guideline. CMAJ. 2020;192(31):E875-E891. doi:10.1503/cmaj.191707
- Longo M, Zatterale F, Naderi J, et al. Adipose tissue dysfunction as determinant of obesity-associated metabolic complications. Int J Mol Sci. 2019;20(9):2358. doi:10.3390/ijms20092358
- Guglielmi V, Morretti T, Morazzini M, Sbraccia P. Fat and lipid partitioning: phenotyping beyond BMI. J Diabetes Endocrinol Metab Disord. 2017:1-6.
- Bray GA, Kim KK, Wilding JPH, World Obesity Federation. Obesity: a chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes Rev. 2017;18(7):715-723. doi:10.1111/obr.12551
- Horn DB, Almandoz JP, Look M. What is clinically relevant weight loss for your patients and how can it be achieved? A narrative review. Postgrad Med. 2022;134(4):359-375. doi:10.1080/00325481.2022.2051366
- Fitch AK, Bays HE. Obesity definition, diagnosis, bias, standard operating procedures (SOPs), and telehealth: an Obesity Medicine Association (OMA) clinical practice statement (CPS) 2022. Obes Pillars. 2022;15:1:100004. doi:10.1016/j.obpill.2021.100004
- Ansari S, Haboubi H, Haboubi N. Adult obesity complications: challenges and clinical impact. Ther Adv Endocrinol Metab. 2020;11:2042018820934955. doi:10.1177/2042018820934955
- Fruh SM. Obesity: risk factors, complications, and strategies for sustainable long-term weight management. J Am Assoc Nurse Pract. 2017;29(S1):S3-S14. doi:10.1002/2327-6924.12510
- Garvey WT. New horizons. A new paradigm for treating to target with second-generation obesity medications. J Clin Endocrinol Metab. 2022;107(4):e1339-e1347. doi:10.1210/clinem/dgab848
- Cefalu WT, Bray GA, Home PD, et al. Advances in the science, treatment, and prevention of the disease of obesity: reflections from a diabetes care editors’ expert forum. Diabetes Care. 2015;38(8):1567-1582. doi:10.2337/dc15-1081
- Chait A, den Hartigh LJ. Adipose tissue distribution, inflammation, and its metabolic consequences, including diabetes and cardiovascular disease. Front Cardiovasc Med. 2020;7:22. doi:10.3389/fcvm.2020.00022
- Ryan DH, Yockey SR. Weight loss and improvement in comorbidity: differences at 5%, 10%, 15%, and over. Curr Obes Rep. 2017;6(2):187-194. doi:10.1007/s13679-017-0262-y
- Romero-Corral A, Caples SM, Lopez-Jimenez F, Somers VK. Interactions between obesity and obstructive sleep apnea: implications for treatment. Chest. 2010;137(3):711-719. doi:10.1378/chest.09-0360
- Garvey WT, Mechanick JI, Brett EM, et al. American Association of Clinical Endocrinologists and American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr Pract. 2016;22(suppl 3):1-203. doi:10.4158/EP161365.GL
- Timper K, Brüning JC. Hypothalamic circuits regulating appetite and energy homeostasis: pathways to obesity. Dis Model Mech. 2017;10(6):679-689. doi:10.1242/dmm.026609
- Roh E, Song DK, Kim M. Emerging role of the brain in the homeostatic regulation of energy and glucose metabolism. Exp Mol Med. 2016;48(3):e216. doi:10.1038/emm.2016.4
- Melby CL, Paris HL, Foright RM, Peth J. Attenuating the biologic drive for weight regain following weight loss: must what goes down always go back up? Nutrients. 2017;9(5):468. doi:10.3390/nu9050468
- Apovian CM, Aronne LJ, Bessesen DH, et al. Pharmacological management of obesity: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2015;100(2):342-362. doi:10.1210/jc.2014-3415
- Evert AB, Franz MJ. Why weight loss maintenance is difficult. Diabetes Spectr. 2017;30(3):153-156. doi.10.2337/ds017-0025
- Sumithran P, Prendergast LA, Delbridge E, et al. Long-term persistence of hormonal adaptations to weight loss. N Engl J Med. 2011;365(17):1597-1604. doi:10.1056/NEJMoa1105816
- Theilade S, Christensen MB, Vilsbøll T, Knop FK. An overview of obesity mechanisms in humans: endocrine regulation of food intake, eating behaviour and common determinants of body weight. Diabetes Obes Metab. 2021;23 (suppl 1):17-35. doi:10.1111/dom.14270
- Rubino F, Puhl RM, Cummings DE, et al. Joint international consensus statement for ending stigma of obesity. Nat Med. 2020;26(4):485-497. doi:10.1038/s41591-020-0803-x
- Anderson JW, Konz EC, Frederich RC, Wood CL. Long-term weight-loss maintenance: a meta-analysis of US studies. Am J Clin Nutr. 2001;74(5):579-584. doi:10.1093/ajcn/74.5.579
- Hall KD, Kahan S. Maintenance of lost weight and long-term management of obesity. Med Clin North Am. 2018;102(1):183-197. doi:10.1016/j.mcna.2017.08.012
- Younossi ZM, Koenig AB, Abdelatif D, et al. Global epidemiology of nonalcoholic fatty liver disease—meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73-84. doi:10.1002/hep.28431